








The Quiet Threat in Your Arteries: Atherosclerotic Cardiovascular Disease Explained
Most people don’t wake up thinking about their arteries. You feel fine, you get through your day, and unless something hurts, it’s easy to assume everything inside is working perfectly. The problem is that some of the most serious health issues develop slowly and silently. Atherosclerotic cardiovascular disease is one of them. It can take years to form, show few obvious signs, and then suddenly become impossible to ignore when it triggers a heart attack, stroke, or circulation problem. The good news is that once you understand what’s happening and why, you can take practical steps to lower risk and protect your future.
What atherosclerotic cardiovascular disease actually is
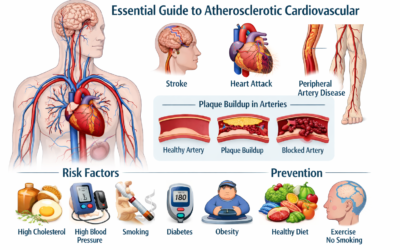
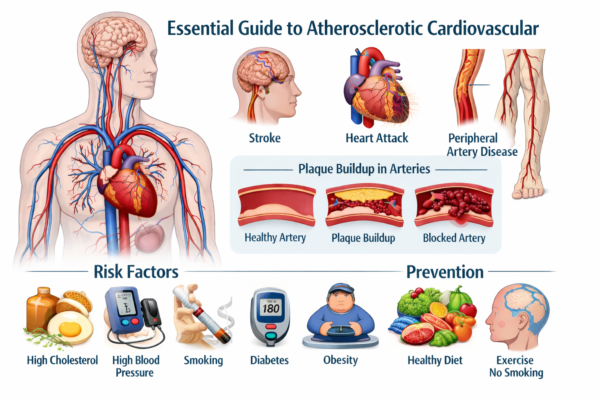
Atherosclerotic cardiovascular disease is a broad term for conditions caused by atherosclerosis, which is the buildup of plaque inside the arteries. Plaque is not just “fat.” It’s a mix of cholesterol, inflammatory cells, calcium, and other substances that collect under the inner lining of artery walls. Over time, this buildup narrows the passage where blood is supposed to flow smoothly. As the artery becomes tighter and less flexible, organs may receive less oxygen-rich blood, especially during activity or stress.
This process doesn’t only affect the heart. It can involve the arteries that supply the brain, kidneys, intestines, and legs. That’s why the effects can look different from person to person. Some people notice chest pressure, others have leg pain when walking, and some don’t notice anything until a major event happens. The real danger is that plaque can become unstable. When a plaque cracks, the body treats it like an injury and forms a clot. That clot can block the artery quickly, turning a slow problem into an emergency.
How plaque builds up over time
To understand atherosclerotic cardiovascular disease, it helps to picture an artery as a flexible tube lined with a smooth inner surface. That lining can be irritated or damaged by things like high blood pressure, cigarette smoke, high blood sugar, and unhealthy cholesterol patterns. Once the lining is disrupted, cholesterol particles can slip into the artery wall. The immune system shows up to “clean up,” which creates inflammation. Inflammation is meant to protect you, but in this situation it can help plaque grow and harden.
As plaque gets larger, blood flow becomes more restricted. At first, the body can compensate by redirecting blood or expanding smaller vessels. That’s why symptoms can be absent early on. But as narrowing worsens, symptoms appear, often when you’re active and your body needs more oxygen. The most dangerous moment is when plaque becomes fragile and ruptures. A sudden clot can fully block an artery, causing a heart attack or ischemic stroke.
Where it shows up in the body

Atherosclerotic cardiovascular disease is often talked about as “heart disease,” but it’s bigger than that. The location of plaque determines the kind of symptoms and complications a person might experience.
If plaque builds in the coronary arteries, it can reduce blood supply to the heart muscle. This may cause angina, which can feel like pressure, squeezing, or heaviness in the chest, especially during exertion or emotional stress. If a clot blocks a coronary artery, it can cause a heart attack.
If plaque affects the carotid or brain arteries, the biggest risk is an ischemic stroke. Warning signs can include sudden weakness on one side of the body, trouble speaking, facial drooping, vision changes, or sudden confusion. These symptoms require urgent care.
If plaque narrows leg arteries, it can cause peripheral artery disease. Many people first notice cramping or aching in the calf or thigh when walking that improves with rest. In more advanced cases, people may have cold feet, numbness, or wounds that heal slowly.
Risk factors that raise the odds
Some risk factors are inherited, and some are tied to lifestyle. Often, it’s the combination that matters most. A person might have “okay” numbers in one area, but multiple mild risks can add up over time.
High LDL cholesterol is a key driver, because LDL particles can contribute to plaque formation. Low HDL cholesterol can also matter, since HDL helps carry cholesterol away from the arteries. High blood pressure increases strain on artery walls and speeds up damage. Smoking directly injures the artery lining and makes blood more likely to clot. Diabetes and insulin resistance raise inflammation and harm blood vessels, which is why cardiovascular risk is higher in people with elevated blood sugar.
Extra weight, especially around the waist, often comes with higher blood pressure, worse cholesterol patterns, and higher glucose. Inactivity makes it harder to control these factors. Poor sleep and chronic stress can quietly push blood pressure up, increase cravings for unhealthy foods, and make consistency harder.
Because atherosclerotic cardiovascular disease develops over years, risk factors matter even when you feel fine. Think of them as long-term pressure on your system, not just a short-term problem.
Symptoms people overlook

Many people expect a heart problem to feel like dramatic chest pain. Real life is often messier. Some symptoms are subtle, especially early on.
For heart-related plaque, symptoms may include chest pressure, shortness of breath, unusual fatigue, nausea, or discomfort that spreads to the shoulder, arm, jaw, neck, or upper back. Some people notice reduced exercise tolerance over time, like getting winded on stairs that used to feel easy.
For brain-related plaque, symptoms may come on suddenly. Even if the symptoms fade quickly, it can be a warning sign. That temporary episode may be a transient ischemic attack, sometimes called a mini-stroke, and it deserves immediate evaluation.
For leg-related plaque, the classic sign is pain while walking that improves with rest. People often blame “getting older” or arthritis, but circulation problems can look similar. Cold extremities, weak pulses, or slow-healing sores can also be signs.
How doctors diagnose it
Diagnosis starts with a conversation and a risk review. A clinician will ask about smoking, activity level, family history, blood pressure, cholesterol, diabetes, and symptoms. Basic tests often include blood pressure measurement and blood work to check cholesterol and blood sugar.
If symptoms suggest reduced blood flow to the heart, a clinician may order an ECG, an exercise stress test, or imaging studies. For possible carotid narrowing, ultrasound is commonly used. For leg circulation, an ankle-brachial index can compare blood pressure at the ankle and arm to screen for peripheral artery disease. In some cases, CT-based imaging may be used to look for calcium buildup or artery narrowing.
The goal of testing isn’t just to label a condition. It’s to identify risk level, determine if symptoms are due to reduced blood flow, and guide a plan that lowers future events.
Lifestyle steps that make a real difference
Atherosclerotic cardiovascular disease is not only managed in hospitals. A huge part of prevention happens in daily routines. The best approach is the one you can do consistently.
Start with food choices that support healthier cholesterol and lower inflammation. Focus meals around vegetables, fruits, beans, lentils, whole grains, nuts, seeds, and healthy fats. Choose lean proteins like fish, chicken, and plant-based options. Reduce processed foods, sugary drinks, and frequent fried meals. This isn’t about perfection. It’s about shifting your “most days” toward foods that help your arteries rather than strain them.
Move more in a way that fits your life. Walking is underrated. Regular brisk walking improves blood pressure, insulin sensitivity, and lipid levels. Strength training also helps by improving metabolism and supporting healthy weight. If you’ve been inactive, start small and build. Consistency beats intensity.
Quit smoking if you smoke. This is one of the most powerful changes you can make. The benefits begin quickly, and within months the body’s circulation and lung function can improve. Many people succeed with a mix of support, counseling, and medication, so it’s worth seeking help rather than trying to push through alone.
Sleep and stress aren’t “extra” topics; they matter. Poor sleep raises hunger hormones, worsens blood pressure, and makes cravings stronger. Chronic stress can create a cycle of emotional eating, inactivity, and sleep problems. Simple habits like fixed sleep times, a short evening wind-down routine, and daily walking can help more than people expect.
Treatment options and why they’re used

For many people, lifestyle changes are the foundation, but medication adds protection, especially if risk is higher or if someone already had an event. The goal is not just improving numbers on a lab report. The goal is lowering the chance of plaque rupture, clot formation, and future emergencies.
Cholesterol-lowering medications, particularly statins, are commonly used because they lower LDL and can help stabilize plaque. In some cases, additional medications may be used if cholesterol remains high despite treatment or if someone has very high risk.
Blood pressure medications reduce strain on artery walls and help protect the heart, brain, and kidneys. For people with diabetes, improving glucose control protects blood vessels, and certain diabetes medications may offer additional cardiovascular benefits. In selected patients, medications that reduce clotting risk may be recommended, particularly after a heart attack, stent placement, or stroke.
If arteries are severely narrowed, procedures may be needed. Stents, bypass surgery, carotid procedures, and treatments for leg arteries are used when symptoms are significant or when a blockage puts a person at high immediate risk. Even when procedures help, long-term prevention still matters, because plaque can develop in other areas if risk factors remain uncontrolled.
Living with it long-term
Atherosclerotic cardiovascular disease often requires a long view. It’s not a one-and-done diagnosis. Many people do well for decades by treating it like a maintenance plan: regular checkups, consistent medication use if prescribed, and steady lifestyle habits that reduce inflammation and stabilize plaque.
One helpful mindset shift is this: the goal is not simply preventing plaque from growing. The goal is stabilizing it so it’s less likely to rupture. That’s why smoking cessation, blood pressure control, cholesterol management, and steady activity are so protective. They work together to reduce the “surprise emergency” risk that people fear most.
Conclusion
Atherosclerotic cardiovascular disease can be quiet for a long time, but it doesn’t have to be a mystery. It’s a process driven by plaque buildup and inflammation, influenced by cholesterol, blood pressure, smoking, blood sugar, and everyday habits. The best protection comes from stacking small wins: a realistic eating pattern, regular movement, smoke-free living, better sleep, and medical treatment when needed. If you have risk factors or a strong family history, take it as a prompt to get checked and build a plan that fits your life. Over time, those consistent steps can reduce risk and protect the heart, brain, and circulation.
FAQs
What is atherosclerotic cardiovascular disease?
Atherosclerotic cardiovascular disease is a group of conditions caused by plaque buildup in arteries that reduces blood flow. It can lead to heart attack, stroke, and circulation problems.
Can atherosclerotic cardiovascular disease be prevented?
Yes, risk can be lowered through healthy eating, regular activity, not smoking, and controlling blood pressure, cholesterol, and blood sugar. Prevention is strongest when habits are consistent.
What are the early signs I should watch for?
Early signs can include chest pressure with activity, shortness of breath, leg pain while walking, or sudden short-lived neurologic symptoms. Many people have no symptoms until the condition is advanced.
Does cholesterol always cause this condition?
High LDL cholesterol is a major contributor, but it’s usually part of a larger picture that includes blood pressure, smoking, diabetes, and inflammation. Multiple risk factors together raise risk more.
How is it treated if I already have it?
Treatment often includes lifestyle changes plus medications to control cholesterol, blood pressure, and clot risk. In severe cases, procedures like stents or bypass surgery may be needed to restore blood flow.
You May Also Read: Stephen Barlow: A Clear, Informational Guide to the Name, Careers, and Public Profiles
